Health consequences of exposure to aircraft contaminated air and fume events: a narrative review and medical protocol for the investigation of exposed aircrew and passengers
There is a need for a systematic and consistent approach to diagnosis and treatment of persons who have been exposed to toxic fumes in aircraft cabins. The medical protocol presented in this paper has been written by internationally recognised experts and presents a consensus approach to the recognition, investigation and management of persons suffering from the toxic effects of inhaling thermally degraded engine oil and other fluids contaminating the air conditioning systems in aircraft, and includes actions and investigations for in-flight, immediately post-flight and late subsequent follow up.
Members (from nine countries) were selected based on clinical, professional and/or academic understanding of specific topics in the field of fume events
UFP measurements in the cabin air identified increased concentrations of UFPs, associated with engine and APU power and air supply changes in phases of flight, and correlating with times when oil seals are less effective enabling oil leakage to occur
This article written in 2023 discusses symptoms and diagnoses of toxic cabin air exposure, the causes of toxic cabin air and studies about how a person is exposed, as well as respiratory/cardiac complaints, neurological complaints, and how the toxicity manifests itself and procedures recommended to use.
Burdon, J., Budnik, L.T., Baur, X. et al. Health consequences of exposure to aircraft contaminated air and fume events: a narrative review and medical protocol for the investigation of exposed aircrew and passengers. Environ Health 22, 43 (2023). https://doi.org/10.1186/s12940-023-00987-8
Link to full article—https://ehjournal.biomedcentral.com/articles/10.1186/s12940-023-00987-8
Quick Reference Guide For Health Care Providers:
Health Impact Of Exposure To Contaminated Supply Air On Commercial Aircraft
afacwa.org
■ Summary: Outside air is bled off the engines/auxiliary power unit and supplied to the cabin/
flight deck on commercial aircraft. Under certain failure conditions, toxicants such as pyrolyzed
en gine oils and hydraulic fluids may leak into the aircraft cabin and flight deck air supply
systems. Air line workers may develop acute and/or chronic health effects and seek attention from
health care
providers. This quick guide focuses on oil exposures. The complete reference guide is available at
www.ohrca.org/healthguide.html.
■ Exposures: The “bleed air” is not filtered and contaminant levels are not monitored. Airborne
toxicants include a complex mixture of oil-based compounds, irritant gases, and ultra-fine
particles. Exposures of particular concern include tricresylphosphates (TCPs) and
N-phenyl-L-naphthylamine (PAN), and carbon monoxide (CO). The primary exposure pathway is
inhalation. Some crewmem bers describe low-level chronic exposures to fumes (e.g., routine and
transient fumes on engine start up); others describe acute, visible fume events, which may result in a flight diversion or
cancellation. Other exposures in the cabin/flight deck include ozone gas, insecticides, deicing fluid,
exhaust and fuel fumes, and cleaning products. Also, the cabin altitude is typically 6,000-8,000
feet inflight, with a corresponding reduction in the partial pressure of oxygen.
■ Documentation: Crewmembers submit written reports of smoke, fumes and/or odor to their airline.
Aircraft mechanical records and pilot log book entries sometimes document air supply con
tamination. Health care providers can request Material Safety Data Sheets for the particular
oil/hy draulic fluid. Ask for the date, flight number, aircraft number, aircraft type, phase of
flight when the problem was noted, whether there was odor or visible smoke/fumes, duration, whether
the aircraft was sprayed with insecticides, and any supplementary documentation from the
airline/mainte
nance regarding cause. Obtain past medical history, occupational history, and family/social health
history.
■ Health Effects: The most common symptoms reported are acute respiratory, neurological, systemic,
and/or psychiatric symptoms. These typically occur within minutes to a few hours follow ing the
contaminated bleed air event. Symptoms vary depending on the duration and magnitude of exposure,
plus individual factors. Chronic and sometimes delayed neurological, psychiatric, respi ratory,
systemic, and dermal symptoms have been reported.
■ Suggested Case Definition: There is either a documented exposure to bleed air con taminants or a
history of flying on aircraft type(s) documented to have an increased risk of air supply
contamination events; and Initial symptoms occur within 48 hours following exposure; and there is
objective documentation of acute and/or persistent respiratory, neurological, systemic, or
psychiatric symptoms. Note that crewmembers with routine, low-level exposures may also develop
chronic symptoms but may not have documented acute, individual exposure events. Symptoms may start
many months or years prior to examination by the HCP. Attempt to identify the exposure and make a
precise diagnosis (e.g., avoid generic terminology such as “inhalation exposure”) based on a
combination of symptoms and objective evidence of health effects (physical examina tion findings
and/or medical tests).
■ Examination: Evaluate for respiratory effects, with attention to mucous membrane erythema and
mucous discharge (upper}, and wheezing, rhonchi and crackles (lower). Neurological exami nation
should be performed, with assessment of cerebellar function, tremor and gait disturbance.
Neuropsychological screening examination may be useful if symptoms suggest cognitive dysfunc tion,
with assessment of short-term memory function, concentration and color vision loss.
■ Lab Data and Other Tests: A blood test for the TCP additives in aviation engine oils is be ing
developed but is not yet available for routine use. Diagnostic tests include: plasma butylcholin
esterase, oxygen saturation, arterial carboxyhemoglobin, \ pulmonary function tests with pre/post
bronchodilators, and chest radiograph. There are currently no tests of sufficient sensitivity and
specificity to definitively assess exposure or other health outcomes. Preliminary research suggests
that tests of the autonomic nervous system and autoantibodies may be useful in evaluating expo
sure and chronic neurotoxicity
■ Treatment: Promptly remove the individual from the aircraft environment and other airborne
contaminants such as diesel exhaust, jet fuel, and cleaning products. Respiratory effects should be
treated according to standard protocols for acute chemical inhalation, including aerosolized
bronchodilators and supplemental oxygen where bronchospasm and/or pneumonitis are present.
The use of intravenous corticosteroids after acute chemical inhalation with bronchospasm may
improve prognosis. Following CO exposure, hyperbaric oxygen may be appropriate. As limited
treatment options are available for neurotoxic injury, some individuals may seek alternative treat
ment techniques. Alternative treatments such as vitamin and nutritional supplementation, nebulized
glutathione, oxygen therapy, yoga, and sauna detoxification are reported by some patients to be of
some benefit. However, these treatments have not been adequately assessed as beneficial in peer
reviewed studies. The HCP should encourage improvement of functional status through exercise,
adequate sleep, well balanced diet, and adequate hydration.
■ Disability Management: Prognosis varies widely. Symptoms often improve and resolve within a few
weeks. If all respiratory, neurological, systemic, and psychiatric symptoms have re solved, the
airline worker can be cleared to return to work on full duty. If symptoms have not com pletely
resolved within two months following one or more contaminated bleed air exposures, the clinician
should consider the likelihood that persistent health effects have occurred. Depending on the
severity, persistent asthma, neurological problems, systemic symptoms (muscle/joint aches,
sensitivity to chemicals, fatigue) and/or psychiatric problems (PTSD, depression, anxiety) may pre
clude the airline worker from return to his/her usual job. Modified duty (such as a ground job) may
be suitable for some crewmembers depending on their functional status.
■ Send correspondence to: Robert Harrison, MD, MPH, University of California, San Francisco,
Division of Occupational and Environmental Medicine, 2330 Post Street, Suite 460, San Francisco, CA
94115; [email protected].
This document is disseminated under the sponsorship of the U.S. Department of Transportation in the
interest of information exchange.
The United States Government assumes no liability for the contents thereof.
Doctor’s guide to pesticide exposure
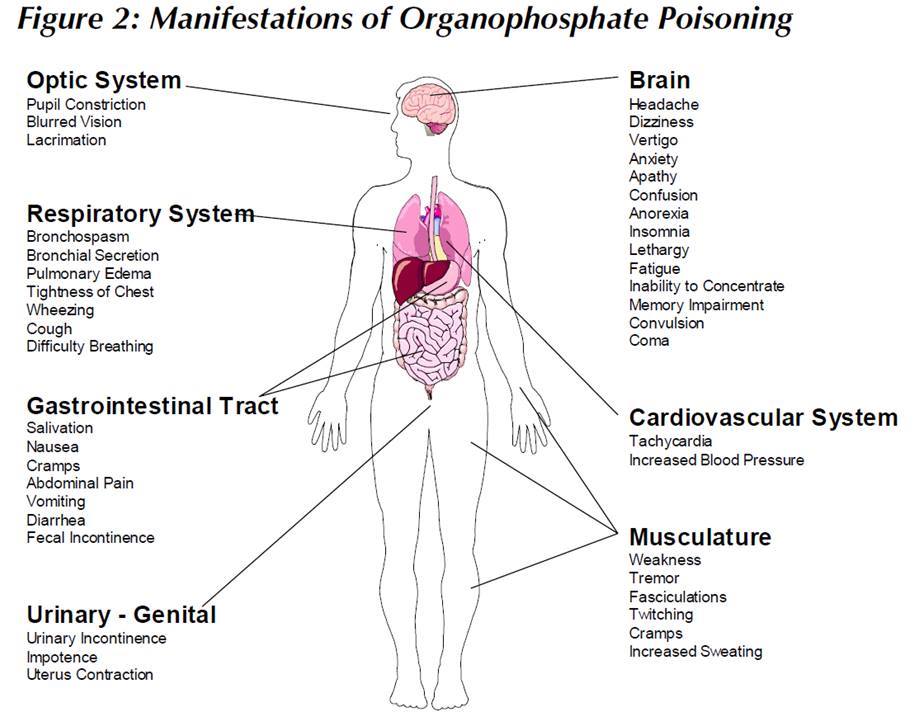
For more information on toxic cabin air visit
www.Aerotoxic.org
The Care Pathway has been developed by an independent working group including experts in toxicology, epidemiology, aviation medicine and primary care, in order to provide advice to health professionals in managing such patients. The working group has also developed an information sheet for patients.
NHS Care Pathway – patients exposed to fumes onboard commercial aircraft
Objective
Crew or passengers who experience symptoms during or following exposure to a fume incident, or symptoms which they think may have been caused by exposure to contaminants in aircraft cabin air, may seek advice from their GP, hospital A & E Dept, occupational health service or Aeromedical Examiner. These doctors may be uncertain how such patients should be assessed or what investigations might be required.
It is important to consider the possibility of underlying disease that is unrelated to exposure to contaminated cabin air, since the symptoms described are generally non-specific and can occur in a range of conditions. People with symptoms should have the same investigations and, if necessary, specialist referral as would be the case for someone with the same symptoms but who had not been exposed to contaminated cabin air.
This care pathway has been developed by the working group to assist doctors in managing such cases.
Background
The cabin air supply on most large commercial aircraft is provided using engine bleed air systems. Fume events – abnormal odours, smoke, haze or fumes in the cabin – may arise from various internal or external sources, and some are due to contamination of the bleed air supply, for example as a result of a failure of an oil seal in the engine. In recent years concerns have been expressed about possible adverse health effects of exposure to contaminants in cabin air.
There is strong evidence that some people experience acute symptoms as a consequence of fume events. Some of the chemical contaminants that are present during such events are irritant, and may cause itching or soreness of the eyes, nasal discharge, sore throat or coughing. In other cases, there may be a psychologically mediated nocebo response (see note) triggered by awareness of irritation or an odour. From the research that has been done to date on the chemicals that may be present in contaminated air, the concentrations at which they are present, and the reported patterns of symptoms in affected individuals, non-irritant toxic mechanisms for the acute health effects seem unlikely.
In addition to the occurrence of acute health effects, a small number of people have attributed longer term illness to one or more contamination incidents or to repeated exposure to lower levels of contamination. However, it is currently unclear whether any form of long-term illness occurs to excess in people with such exposures, and if so, whether it arises through toxic or nocebo mechanisms. From what is currently known about the concentrations of potentially toxic chemicals in contaminated air, long-term toxic effects would not be expected, but this remains an area of scientific uncertainty. (see Further reading 1,2)
Nocebo effect Note: Illness, often with physical symptoms and signs, which is triggered through psychological processes in response to a perceived harmful exposure. The phenomenon is analogous to a placebo effect in which symptoms improve in response to a perceived beneficial exposure.